Journal of Clinical and Biomedical Sciences
DOI: 10.58739/jcbs/v16i1.25.244
Year: 2026, Volume: 16, Issue: 1, Pages: 29-33
Original Article
Ranjan Agrawal1*, Zaheer Ahmad2, Yumkhaibam Sadaki2, Shashwat Verma3
1Professor & Head Pathology, Rajshree Medical Research Institute, Rajshree Medical Research Institute, India.
2Postgraduate student, Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India.
3Assistant Professor, Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India
*Corresponding Author
Email: [email protected]
Received Date:24 May 2025, Accepted Date:24 October 2025, Published Date:31 March 2026
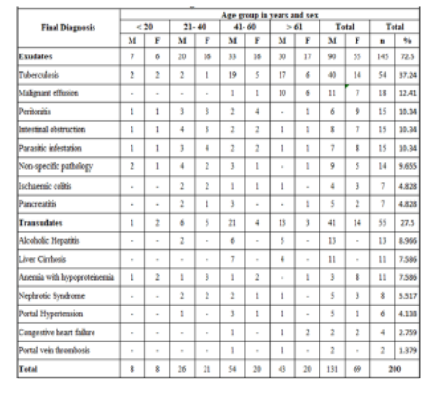
Background: Ascites is a common clinical problem resulting from certain abdominal or systemic diseases. The effusion is likely to be exudative or transudative in nature. Biochemical parameters, serological markers and cytology are used in classifying ascites. Combination of the clinical and cytological findings along with the biochemical parameters help in assessing the cause of these effusions. Materials and Methods: Two hundred fluid samples from cases presenting with ascites along with their simultaneous serum were collected and analysed for different parameters. The ascitic fluid was further studied for biochemical parameters including protein, albumin, glucose, cholesterol, Alkaline Phosphate, bilirubin, amylase, cell counts total and differential, Gram’s stain and, Modified Ziehl-Neelsen stain for AFB based on which they were categorised into different groups. Serum samples were also assayed for protein, albumin, bilirubin, cholesterol and amylase levels. SAAG was used to assess the type of ascites. Results: Of these 200 samples, 145 (71.2%) were exudates and 55(28.8%) were transudates. There were 131 males and 69 females, with a M:F ratio of 1.90:1. Tuberculosis followed by peritonitis and malignancy were amongst the common etiologies seen in exudative effusions. Among transudates, alcoholic hepatitis followed by liver cirrhosis and anaemia with hypoproteinaemia were the commonest cause observed.
Keywords: Effusion, SAAG Biochemical, Exudate, Transudate
1. Agarwal R, Panesar A, Lewis RR. Dipstick proteinuria: Can it guide hypertension management?. American Journal of Kidney Diseases. 2002; 39 (6). Available from: https://doi.org/10.1053/ajkd.2002.33389
2. Gupta R, Misra SP, Dwivedi M, Misra V, Kumar S, Gupta SC. Diagnosing ascites: Value of ascitic fluid total protein, albumin, cholesterol, their ratios, serum‐ascites albumin and cholesterol gradient. Journal of Gastroenterology and Hepatology. 1995; 10 (3). Available from: https://doi.org/10.1111/j.1440-1746.1995.tb01096.x
3. Moore KP, Aithal GP. Guidelines on the management of ascites in cirrhosis. Gut. 2006; 55 (suppl 6). Available from: https://doi.org/10.1136/gut.2006.099580
4. Elis A, Meisel S, Tischler T, Kitai Y, Lishner M. Ascitic Fluid to Serum Bilirubin Concentration Ratio for the Classification of Transudates or Exudates. American Journal of Gastroenterology. 1998; 93 (3). Available from: https://doi.org/10.1111/j.1572-0241.1998.00401.x
5. European Association for the Study of the liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. Journal of Hepatology. 2010; 53 (3). Available from: https://doi.org/10.1016/j.jhep.2010.05.004
6. Moore KP, Wong F, Gines P, Bernardi M, Ochs A, Salerno F, <I>et al</I>. The Management of Ascites in Cirrhosis: Report on the Consensus Conference of the International Ascites Club. Hepatology. 2003; 38 (1). Available from: https://doi.org/10.1053/jhep.2003.50315
7. Alexandrakis MG, Moschandrea JA, Koulocheri SA, Kouroumalis E, Eliopoulos GD. Discrimination Between Malignant and Nonmalignant Ascites Using Serum and Ascitic Fluid Proteins in a Multivariate Analysis Model. Digestive Diseases and Sciences. 2000; 45 (3). Available from: https://doi.org/10.1023/a:1005437005811
8. Runyon BA, Montano AA, Akriviadis EA, Antillon MR, Irving MA, MC Hutchinson JG. The Serum-Ascites Albumin Gradient Is Superior to the Exudate-Transudate Concept in the Differential Diagnosis of Ascites. Annals of Internal Medicine. 1992; 117 (3). Available from: https://doi.org/10.7326/0003-4819-117-3-215
9. Bendtsen F, Grønbaek H, Hansen JB, Aagaard NK, Schmidt L, Møller S. Treatment of ascites and spontaneous bacterial peritonitis - Part I. <I>Danish Medical Journal</I> 2012;59:C4371.
10. Topal NB, Gurel S, Ercan I, Savci G. The role of ultrasonography and computed tomography in determining the etiology of ascites. <I>Saudi Medical Journal</I>. 2007;28(12):1822-6.
11. Yamada T, Alpers DH, Kaplowitz N. Approach to the patient with ascites. <I>Textbook of Gastroenterology</I>. 2003;1:948–72.
12. Selvaraju K, Sridevi M. Analysis of ascitic fluid in differentiating transudate versus exudate - in a tertiary care centre. Indian Journal of Pathology and Oncology. 2020; 7 (1). Available from: https://doi.org/10.18231/j.ijpo.2020.026
13. Arroyo V. Pathophysiology, diagnosis and treatment of ascites in cirrhosis. Annals of Hepatology. 2002; 1 (2). Available from: https://doi.org/10.1016/s1665-2681(19)32178-7
14. Biecker E. Diagnosis and therapy of ascites in liver cirrhosis. World Journal of Gastroenterology. 2011; 17 (10). Available from: https://doi.org/10.3748/wjg.v17.i10.1237
15. Cardenas A, Gines P. Management of refractory ascites. <I>Clinical Gastroenterology and Hepatology</I> 2005;3:1187–91.
16. Gotyo N, Hiyama M, Adachi J, Watanabe T, Hirata Y. Respiratory Failure with Myxedema Ascites in a Patient with Idiopathic Myxedema. Internal Medicine. 2010; 49 (18). Available from: https://doi.org/10.2169/internalmedicine.49.3923
17. Dıaz-Mancebo R, Sanchez-Villanueva R, Gonzalez-Garc´ıa E, Ossorio- Gonzalez M, Selgas-Gutierrez R. Nephrogenic ascites: a thing of the past? <I>Nefrologia</I> 2012;32:406–8.
18. Gines P, Cardenas A. The Management of Ascites and Hyponatremia in Cirrhosis. Seminars in Liver Disease. 2008; 28 (1). Available from: https://doi.org/10.1055/s-2008-1040320
19. Hoefs JC. Serum protein concentration and portal pressure determine the ascitic fluid protein concentration in patients with chronic liver disease. <I>Journal of Laboratory and Clinical Medicine</I> 1983;102:260–73.
20. Uddin MS, Hoque MI, Islam MB. Serum-ascites albumin gradient in differential diagnosis of ascites. <I>Mymensingh Medical Journal</I>. 2013;22(4):748–54.
21. Romero S, Candela A, Martin C, Hernadez L, Trigo C, Gil J. Evaluation of Different Criteria for the Separation of Pleural Transudates From Exudates. Chest. 1993; 104 (2). Available from: https://doi.org/10.1378/chest.104.2.399
22. Tarn AC, Lapworth R. Biochemical analysis of ascitic (peritoneal) fluid: what should we measure?. Annals of Clinical Biochemistry: International Journal of Laboratory Medicine. 2010; 47 (5). Available from: https://doi.org/10.1258/acb.2010.010048
23. Senousy BE, Dragnov PV. Evaluation and management of patients with refractory ascites. World Journal of Gastroenterology. 2009; 15 (1). Available from: https://doi.org/10.3748/wjg.15.67
24. Singhal S, Baikati KK, Jabbour II, Anand S. Management of Refractory Ascites. American Journal of Therapeutics. 2012; 19 (2). Available from: https://doi.org/10.1097/mjt.0b013e3181ff7a8b
25. Milevoj KL, Culej J, Jokic A, Bozovic M, Kocijan I. Laboratory testing of extravascular body fluids: National recommendations on behalf of Croatian society of medical biochemistry and laboratory medicine Part 1- Serous fluids. Biochemia medica. 2020; 30 (1). Available from: https://doi.org/10.11613/bm.2020.010502
26. Aravindan R, KH Noorul Ameen, Comparison of the Diagnostic Accuracy of Serum Ascites Albumin Gradients (SAAG) With the Traditional Marker-Ascitic Fluid Total Protein. <I>Journal of Research in Medical and Dental Science</I>. 2021, 9 (5):271-5.
27. Puste S, Swetha P, Alivelu T, Mona D. A clinical study to prove that serum ascites albumin gradient has superior discriminating power over ascitic fluid total protein in classifying portal and non portal causes of ascites. <I>International Journal of Medical Science and Public Health Research</I>. 2024; 14 (3); 607-11.
28. Kumar NA. A study on ascitic fluid total protein and serum ascites albumin gradient in evaluation of ascites in children. <I>International Journal of Health and Clinical Research</I> 2021: 4(19), 350-4.
29. Vadlapudi SS, Srivastava A, Saini N, Sen SM, Poddar U, Yachha SK. Aetiology and diagnostic utility of serum ascites albumin gradient in children with ascites. Digestive and Liver Disease. 2024; 56 (9). Available from: https://doi.org/10.1016/j.dld.2024.02.004
30. Reddy BS, Srinivasa D, Kumar S. Diagnostic Accuracy of Serum Ascites Albumin Gradient (SAAG) with Ascitic Fluid Total Protein (AFTP) in Determining the Etiopathogenesis of Ascites. International Journal of Pharmaceutical and Clinical Research. 2024; 16(10); 901-5
31. Subhani M, Sheth A, Palaniyappan N, Sugathan P, Wilkes EA, Aithal GP. Diagnostic accuracy of serum ascites albumin gradient (SAAG) in a contemporary unselected medical cohort. Journal of International Medical Research. 2022; 50 (11). Available from: https://doi.org/10.1177/03000605221140310
32. Sandeesha V, Kiran CR, Ushakiran P, Sulemani MD, Lakshmanakumar N. A comparative study of serum effusion albumin gradient and Light's criteria to differentiate exudative and transudative pleural effusion. Journal of Family Medicine and Primary Care. 2020; 9 (9). Available from: https://doi.org/10.4103/jfmpc.jfmpc_321_20
33. Runyon BA. Management of adult patients with ascites due to cirrhosis. Hepatology. 2009; 49 (6). Available from: https://doi.org/10.1002/hep.22853
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Published By Sri Devaraj Urs Academy of Higher Education, Kolar, Karnataka
Subscribe now for latest articles and news.